Paediatric Surgery Curriculum
3 Programme of Learning
This section covers the expected learning outcomes, learning methods, breadth of experience and levels of performance at critical progression points in the training programme and the levels of performance expected of those completing training.
3.1 What has to be learnt to complete the curriculum
The practice of Paediatric Surgery requires the generic and specialty knowledge, clinical and technical skills and behaviours to manage patients presenting with a wide range of congenital and acquired conditions in infants and children. It involves development of competence in diagnostic reasoning, managing uncertainty, dealing with co-morbidities, and recognising when another specialty opinion or care is required (as well as developing technical skills in the areas and to the level described in the syllabus as shown in appendix 2). The main areas for learning are described by the CiPs which are the high-level learning outcomes for training in Paediatric Surgery described below and shown in full in appendix 1.
3.2 Capabilities in Practice (the high-level outcomes of training)
Training is designed to produce a person capable of safely and effectively performing the role of a first day consultant surgeon. The role of a consultant surgeon can be thought of as a sum of all the various tasks which need to be performed through a working week. These tasks are the high-level outcomes of the curriculum and grouping these together describe the role of a consultant surgeon. To perform a high-level clinical task as a consultant surgeon requires trainees to be able to integrate areas of learning from all parts of the syllabus, including knowledge, clinical skills, professional skills and technical skills. In addition, a consultant surgeon will need to have acquired the generic skills, behaviours and values shared by all doctors in order to perform this task safely and well. A capability is a set of skills that can be developed through training from novice to expert and, therefore, these high-level clinical outcomes are known as Capabilities in Practice. They are common across all surgical specialties and are delivered within the context of the GPCs and the specialty syllabus.
There are five CiPs which are shared between all surgical specialties:
- Manages an out-patient clinic
- Manages the unselected emergency take
- Manages ward rounds and the on-going care of in-patients
- Manages an operating list
- Manages multi-disciplinary working
- Assesses and manages an infant or child in a NICU/PICU environment*
*In addition to these, the Paediatric Surgery specialty-specific CiP
The generic knowledge, skills, behaviours and values shared by all doctors are described in the GPC framework. The GPCs are essential components and have equal weight to the CiPs in the training and assessment of clinical capabilities and responsibilities in the training programme.
The GPC framework has nine domains:
Domain 1: Professional values and behaviours
Domain 2: Professional skills
Practical skills
Communication and interpersonal skills
Dealing with complexity and uncertainty
Clinical skills
Domain 3: Professional knowledge
Professional requirements
National legislative requirements
The health service and healthcare system in the four countries
Domain 4: Capabilities in health promotion and illness prevention
Domain 5: Capabilities in leadership and team working
Domain 6: Capabilities in patient safety and quality improvement
Patient safety
Quality improvement
Domain 7: Capabilities in safeguarding vulnerable groups
Domain 8: Capabilities in education and training
Domain 9: Capabilities in research and scholarship
Simply put, the CiPs and GPCs are the constituent parts of the role of a consultant surgeon. Each part is as important as the next and doctors are required to be capable in all parts of the role in order to be able to practice independently. In order to complete training and be recommended to the GMC for certification and entry to the specialist register, the doctor must demonstrate that they are capable of unsupervised practice in all the CiPs and GPCs. For example, managing the unselected emergency take (CiP 2), requires the integration of knowledge, clinical and diagnostic skills and technical skills described in the syllabus as well as communication and interpersonal skills, time management skills and many other generic skills described in the GPCs in order to be delivered safely, professionally and effectively. This will be assessed using the Multiple Consultant Report (MCR) as described below. The full content of the six CiPs can be found in appendix 1.
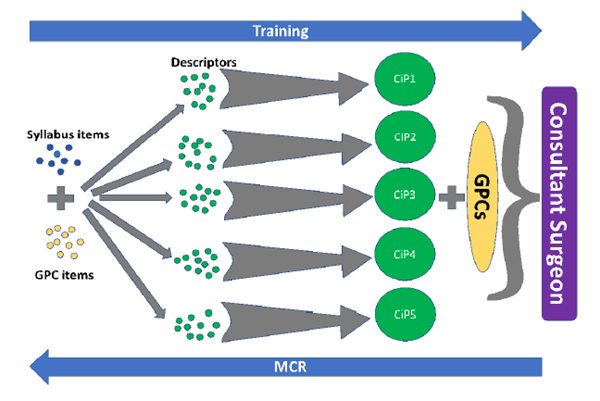
Figure 2 - The interrelationship of the GPCs, the syllabus, the CiPs and their descriptors to the role of a consultant surgeon. Items from the syllabus are combined with items taken from the GPC framework to form the small tasks which are the CiP descriptors. When the small tasks of the descriptors are integrated they comprise the constituent parts of the role of a consultant surgeon (the CiPs). When the CiPs are taken together, along with the GPCs, the role of a consultant surgeon (the overall outcome of the curriculum), is described. Each of these CiPs will be developed through training until the level required of a day-one consultant is reached. Assessment in an outcomes-based curriculum through the MCR examines the trainee from the perspective of the outcome (a consultant surgeon), and compares performance in each CiP and in the GPCs to that level. If the outcome level is not reached, then targeted feedback and development plans can be made with reference to the CiP descriptors and beyond to the syllabus items and GPC items that combine to form the descriptors.
3.3 Descriptors for CiPs
The six CiPs taken together describe the role of a consultant paediatric surgeon but more detail is needed to help trainees develop that capability through training via detailed feedback and focused development goals.
We can break the CiPs down into smaller tasks. Each of these smaller tasks is a CiP descriptor. For example, managing the unselected emergency take (CiP 2), includes the need to promptly assess acutely unwell and deteriorating patients and deliver resuscitative treatment and initial management and ensure sepsis is recognised and treated in compliance with protocol (see appendix 1). If a trainee has not yet reached the level required of a new consultant in a CiP then the descriptors can be used to describe in standard language what needs to be improved through learning and training to allow the trainee to get closer towards the outcome of training. By describing the component parts of a CiP, descriptors also aid decisions on assessment of the level of supervision required by a trainee at the time of that assessment, providing prompts for feedback of performance by allowing identification of areas of excellence or specific detail on areas for development, including in behavioural and professional domains. Descriptors can, therefore, help trainees identify where to focus their efforts to become competent and safe independent practitioners. More detail about assessment and feedback is given in section 5, Programme of Assessment.
Each CiP is judged against a scale that describes the level of supervision required to perform the CiP to the standard of certification. The level of supervision changes in line with the trainee’s progression, consistent with safe and effective care for the patient. Typically, there should be a gradual reduction in the level of supervision required and an increase in the complexity of cases managed until the level of competence for independent practice is acquired. In the early years, therefore, it would be normal for trainees to achieve a lower supervision level and progress as experience is gained.
The supervision levels are:
Level I: Able to observe only
Level II: Able and trusted to act with direct supervision:
a) Supervisor present throughout
b) Supervisor present for part
Level III: Able and trusted to act with indirect supervision
Level IV: Able and trusted to act at the level expected of a day-one consultant
Level V: Able and trusted to act at a level beyond that expected of a day-one consultant
3.4 Critical progression points
Table 1 shows the indicative levels of supervision to be achieved to complete phase 2 and the supervision levels required by the end of phase 3. A trainee becomes eligible for certification when supervision level IV has been achieved in each of the shared and specialty-specific CiPs as well as acquiring all of the skills described in the GPC framework (in addition to the other certification requirements shown in section 5.4) as confirmed by an ARCP panel.
| Capability in practice (shared) |
Indicative Supervision Level (end of phase 2) |
Supervision Level (end of phase 3 and certification) |
| 1. Manages an out-patient clinic |
Level III |
Level IV |
| 2. Manages the unselected emergency take |
Level III |
Level IV |
| 3. Manages ward rounds and the on-going care of in-patients |
Level III |
Level IV |
| 4. Manages an operating list |
Level III |
Level IV |
| 5. Manages multi-disciplinary working |
Level III |
Level IV |
Specialty-specific CiP:
Table 1: Supervision levels to be achieved by the end of each phase of training
| 6. Assesses and manages an infant or child in a NICU/PICU environment |
Level III |
Level IV |
3.5 Breadth of experience required during training
The curriculum requires trainees to accrue a rich experience that promotes deep learning of knowledge, clinical skills, technical skills, professional behaviour, leadership and all other generic professional skills that are considered necessary to ensure patient safety throughout the training process and specifically at the end of training. The scope of practice of a day-one consultant is described in the syllabus. In addition, there are certain skills and conditions within the syllabus that are of such central and fundamental importance to the safe practice of Paediatric Surgery that they are highlighted as critical conditions and index procedures.
3.5.1 The syllabus
The syllabus, shown in appendix 2, provides a detailed description of the specialty-specific knowledge, clinical and technical skills required for each phase of training and for certification. The syllabus is organised by topics which are the presenting conditions of patients in relation to the specialty. Trainees are expected to have exposure to all topics in phase 2 of training.
3.5.2 Critical conditions
From the syllabus, a list of critical conditions has been identified which are of significant importance for patient safety and demonstration of a safe breadth of practice. Across surgery, these are defined as any condition where a misdiagnosis could be associated with devastating consequences for life or limb. These critical conditions are assessed individually by means of the Case Based Discussion (CBD) and Clinical Evaluation Exercise (CEX), which both include an assessment of clinical judgement and decision-making. They provide formative feedback to the trainee and feed into the summative assessment of the Assigned Educational Supervisor (AES) via the AES report for the Annual Review of Competence Progression (ARCP). A list of critical conditions is given in appendix 3. These critical conditions were decided following wide consultation with clinicians and trainers in the specialty.
3.5.3 Index procedures
In addition to the critical conditions, a list of index procedures has been identified. Index procedures are common but important operations central to the specialty, competence in which is essential to the delivery of safe patient care. Taken together they form a representative sample of the breadth of operative procedures in the specialty. Learning in the index procedures is indicative of learning in the broad range of technical procedures in the syllabus and surgical logbook and is, therefore, of significant importance for patient safety and demonstration of a safe breadth of practice. Each of these index procedures is assessed individually by means of the Procedure Based Assessment (PBA) which provides formative feedback to the trainee and feeds into the summative AES report for the ARCP. A list of index procedures expected for Paediatric Surgery is given in appendix 4. These include indicative numbers of cases necessary before certification as trainees would not normally be expected to have achieved sufficient experience to be able to manage the range of pathology they encounter unless these numbers were met. It is recognised that competence could be achieved with fewer cases, if supported by evidence from other assessments. Meeting the numbers does not, in itself, imply competence. These index procedures and indicative numbers were decided following wide consultation with clinicians and trainers in the specialty.
The certification requirements, shown in section 5.4, summarise the experience trainees need to achieve by the end of the training programme.